

By Extension
Patent Term Extensions, Polymorphs, and Drug Performance make this company an attractive bet

There’s no question that biotech names are beaten down. Between interest rates and the IRA, the headwinds have been rough, with IBB 0.00%↑ up less than 18% in the last 5 years and XBI 0.00%↑ up a measly ~5%. Outside of Liquidia though, I have generally stayed away from individual drug development companies, since I’m not a biotech expert. Instead, my largest biotech positions have been on the “picks and shovels” side with Evotec and Charles River.
But some recent patent law-related developments have me diving back into one drug development company in particular.
DISEASE BACKGROUND
Transthyretin amyloid cardiomyopathy (ATTR-CM) is a rare disease in which TTR proteins produced in the liver fold improperly. These proteins, when functioning normally, transport retinol and thyroxine to the liver. In patients with ATTR-CM, the proteins are unstable, and when folded, create tetramer clumps that then group together to form amyloid fibrils. The fibrils “clog up” organs and nerves all over the body, but most significantly in the heart where they eventually cause heart failure. The disease is often called “wild type” cardiomyopathy because it doesn’t usually involve a mutation of the underlying TTR gene, resulting in a sort of spontaneous folding issue whose causes are still unknown, though are certainly age-related (average age of diagnosis: 74).
About 120,000 people have ATTR-CM in the U.S., with about 5,000 to 7,000 new cases diagnosed each year. But this number is almost certainly an underestimate for reasons we’ll get to. That makes ATTR-CM an “orphan disease” (any disease affecting <200,000 people in the U.S.).
For patients with ATTR-CM, early detection is critical. There is no drug on the market (or in development, to my knowledge) which can reverse the effects of these fibril buildups or remove the fibrils from organs and nerves. It’s possible gene editing (e.g., Intellia) and antibody treatments (e.g. Novo) could provide a next-generation option for patients, but neither are near commercialization. Instead, current treatment is focused on stabilization—stabilization of disease progression and literal stabilization of the TTR proteins to prevent them from folding. The earlier patients begin treatment, the better their quality of life and the longer their expected lifespan will be. You can think of it kind of like an infection that starts in your finger and spreads into your hand and up your arm. You’re not aiming to keep the finger. You’re aiming to not lose your arm. Unfortunately for patients, the symptoms look a lot like just about every other form of heart disease, so by the time patients are diagnosed with ATTR-CM, the disease has usually progressed substantially and irreparably. That fact plays a huge role in the low estimates for patient population, as many patients simply go undiagnosed.
CURRENT TREATMENT OPTIONS
Although no existing treatment can remove fibrils from affected organs, patients with ATTR-CM are not without options.
The incumbent treatment for the disease is a drug called Tafamidis, owned by FoldRx (itself a wholly owned subsidiary of Pfizer since 2010) and developed in conjunction with researchers at the Scripps Research Institute. The crowning clinical trial for Tafamidis was the 2018 ATTR-ACT trial, which showed Tafamidis was successful at reducing hospitalizations, reducing deterioration in the 6MWD test and reducing deterioration in quality of life. Unfortunately, the test also reflected substantial unmet need in the market. 70 months after the conclusion of the trial, 50% of patients had died and over 70% of those were cardiovascular-related deaths. In other words, while you’d expect a certain number of deaths in patients at or above 80 years old, the cause of death was commonly linked to the disease progression.
Tafamidis comes in two forms: VYNDAMAX and VYNDAQEL. The former is a free acid version of Tafamidis taken as a single pill per day. The latter is Tafamidis meglumine, a micronized salt form of Tafamidis which is taken by four pills daily. VYNDAMAX was developed as a more convenient form of VYNDAQEL for obvious reasons.

Tafamidis is known as a “stabilizer” because it literally binds to a pocket on the TTR protein as the proteins form tetramers and prevents the proteins from falling apart, as noted above.
OTHER TREATMENTS
Stabilizers
On November 23, BridgeBio obtained FDA approval for its ATTR stabilizer Acoramidis. Acoramidis works in a similar fashion to Tafamidis (it’s also another oral medication); however it binds to a different “pocket” or binding site within the TTR tetramers. This binding site was discovered after researchers in Portugal found that certain individuals have a “super-stabilizing” T119M mutation that prevent patients from developing ATTR-CM, or which at least mitigate symptoms in the event patients have other genetic anomalies causing protein misfolding.
The results for patients in the Acoramidis clinical trials have been stellar, with Acoradmidis being labeled a “complete stabilizer” (i.e., halting progression of the disease vs. Tafamidis’s slowing progression of the disease). The phase 3 trial, the “ATTRibute” trial, showed substantial benefits in hospitalizations, mortality, and 6MWD over the placebo, though interestingly the placebo group showed some slowed progression as compared to baseline progression rates over the course of the trial as well. This is likely due to the fact that, as disease awareness has grown, patients have been diagnosed earlier and earlier, so placebo improvements could be due to changes in these patients’ lifestyle and the mere fact that patients are aware of the disease at an earlier point in the progression curve, which account for the pace of disease progression. Given this is a disease of accumulation, the earlier stages of the disease progress slowly and then increase exponentially, so we’d expect slower progression in 6 months after diagnosis for a patient diagnosed at age 60 as compared to a patient diagnosed at age 75.
Acoramidis, as the “complete stabilizer,” is likely the superior drug over Tafamidis, but it’s critical to caveat that there hasn’t actually been a head-to-head study. Further still, the ACT and ATTRibute clinical trials are hard to compare because of that change in the patient population profile attributable to the drastic change in age of diagnosis. Notably, both Acoramidis and Tafamidis seem to be well-tolerated drugs. The drugs target these “pockets” in the TTR tetramers and only target those pockets. As a result, adverse events and side-effects on the drugs are low. Tafamidis has certain limited interactions with other drugs and statins, but that’s about it.
Silencers
A different way to treat ATTR-CM is to “silence” the production of the TTR protein. Critically, this is another “slow it down” or “stop it in its tracks” treatment, and like the stabilizers, this is not a disease reversal treatment.
The leading company in this space right now is Alnylam. Alnylam’s drug, Vutrisiran has indicated positive results in their phase 3 HELIOS-B trial. Despite the fact that the drug stops production of the TTR protein, the protein’s relatively small role in thyroxine transport, combined with the fact that patients can probably supplement treatment with vitamin A if needed for retinol replacement, means the drug has also been well-tolerated in clinical trials.
Still, the drug is administered via a once-every-3-month subcutaneous injection, meaning patient compliance is a concern. The company is working on a once-every-12-month injection, but has not had approval yet.
Combination Therapies
There is an open question of whether or not stabilizers and silencers can be used in combination. AstraZeneca and Ionis have teamed up in the “Cardio-TTRansform” study to evaluate whether Ionis’s Eplontersen TTR silencer will be effective in combination with stabilizers. Results are expected next year.
But even if the trials show promise, and assuming generic stabilizers hit the market in 2025 (we’ll get to that below), I’m not entirely sure silencer + generic stabilizer wins over top-shelf stabilizer. It’s sort of hard to beat “complete stabilization” as is the case with Acoramidis. Just because Tafamidis generics put pricing pressure on Pfizer doesn’t necessarily mean they’ll have the same effect on Acoramidis sales. Sure, I’d expect some hit to Acoramidis pricing, but there will still be folks who will pay for the better treatment option, even if payers aren’t covering all of the costs.
Still, because they’re separate mechanisms of action, it’s highly likely that the AstraZeneca trial will reveal slowed progress over Tafamidis-only clinical trials, and some doctors will want to prescribe both for patients progressing on a stabilizer alone.
2025-2027 Market
The takeaway here is that, assuming no major changes to the market (which we discuss below), the ATTR-CM market is soon to be a 4-player market:
Pfizer (Tafamidis & Tafamidis meglumine) — Stabilizer
BridgeBio (Acoramidis) — Stabilizer
Alynlam (Vutrisiran) — Silencer
AstraZeneca (Eplontersen) — Silencer
PATENT LANDSCAPE
Despite the fact that there are numerous companies pursuing treatments in the space, we’re going to be talking about Pfizer’s Tafamidis-related patent portfolio today for reasons we’ll get to momentarily.
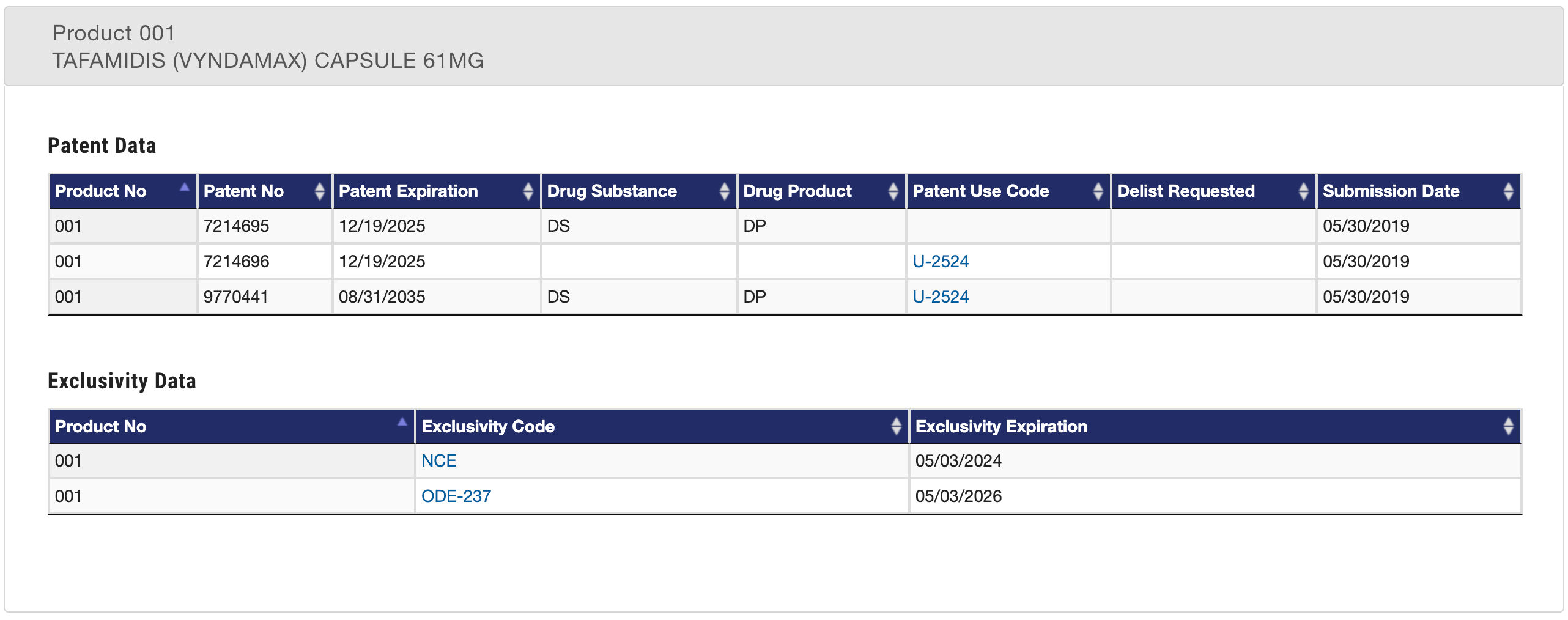
What patents does Pfizer have? A few different patents which variously apply to VYNDAQEL and/or VYNDAMAX. Taking a look at the Orange Book, we can see the associated patents and their respective loss of exclusivity (“LOE”) dates.
VYNDAMAX Exclusivity:
VYNDAQEL Exclusivity:
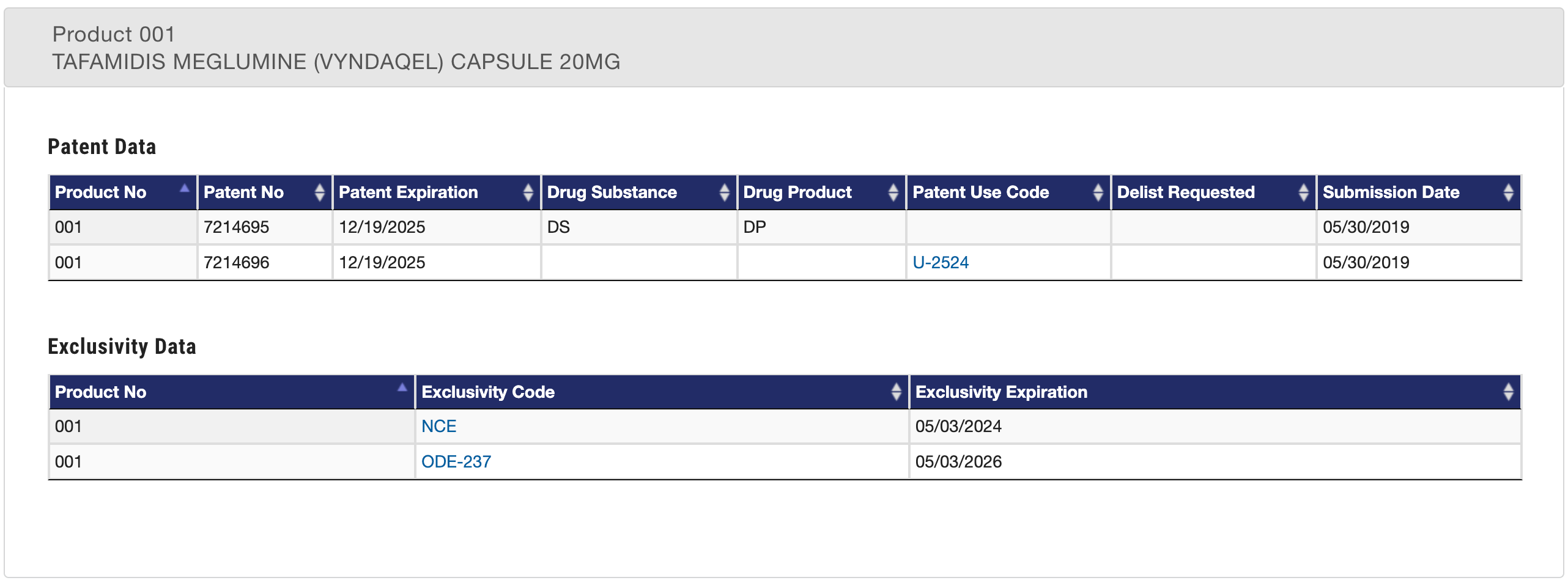
You’ll note that both the 7,214,695 (“the ’695 patent”) and the 7,214,696 (“the ’696 patent”) are listed for both VYNDAMAX and VYNDAQEL. These patents are both directed to “compositions and methods for stabilizing transthyretin and inhibiting transthyretin misfolding” and contain the same patent specification (i.e., same patent family).
The VYNDAMAX exclusivity includes one additional patent—the 9,770,441 patent (“the ’441 patent). This patent is directed to crystalline solid forms of 6-carboxy-2-(3,5-dichlorophenyl)-benzoxazole (i.e., the patent discloses a specific crystalline polymorph form of Tafamidis).